CAR-T cell therapies are transforming cancer treatment, especially for blood cancers, with growing advances in solid tumours through innovative engineering and clinical strategies. These therapies harness genetically modified T cells to target tumour antigens and activate immune responses effectively.

Dr Emilio Cosimo
Scientific Director of Innovation

 Technical Presentations
Technical Presentations|
August 18, 2025
|
7 min read
Chimeric Antigen Receptor (CAR)-T cell therapies have transformed blood cancer treatment and are making advances in solid tumours. This ground-breaking approach has achieved remarkable success in certain blood cancers, delivering high remission rates even in patients who failed standard therapies1,2. CAR-T cells have been called “living drugs” for their ability to persist and fight cancer inside the body. Their strength lies in precise targeting of tumour-associated antigens and activating the immune system at scale.
As research evolves, engineering breakthroughs are overcoming key challenges like antigen heterogeneity and immune suppression. In this post, we take a deeper look at how CAR-T cells work, their clinical impact in oncological indications, and the advanced technologies expanding their potential. We are also sharing two CAR-T case studies in the slide deck with you in case you’d like more details about how the potential of CAR-T cells can be harnessed for novel immunotherapy approaches.
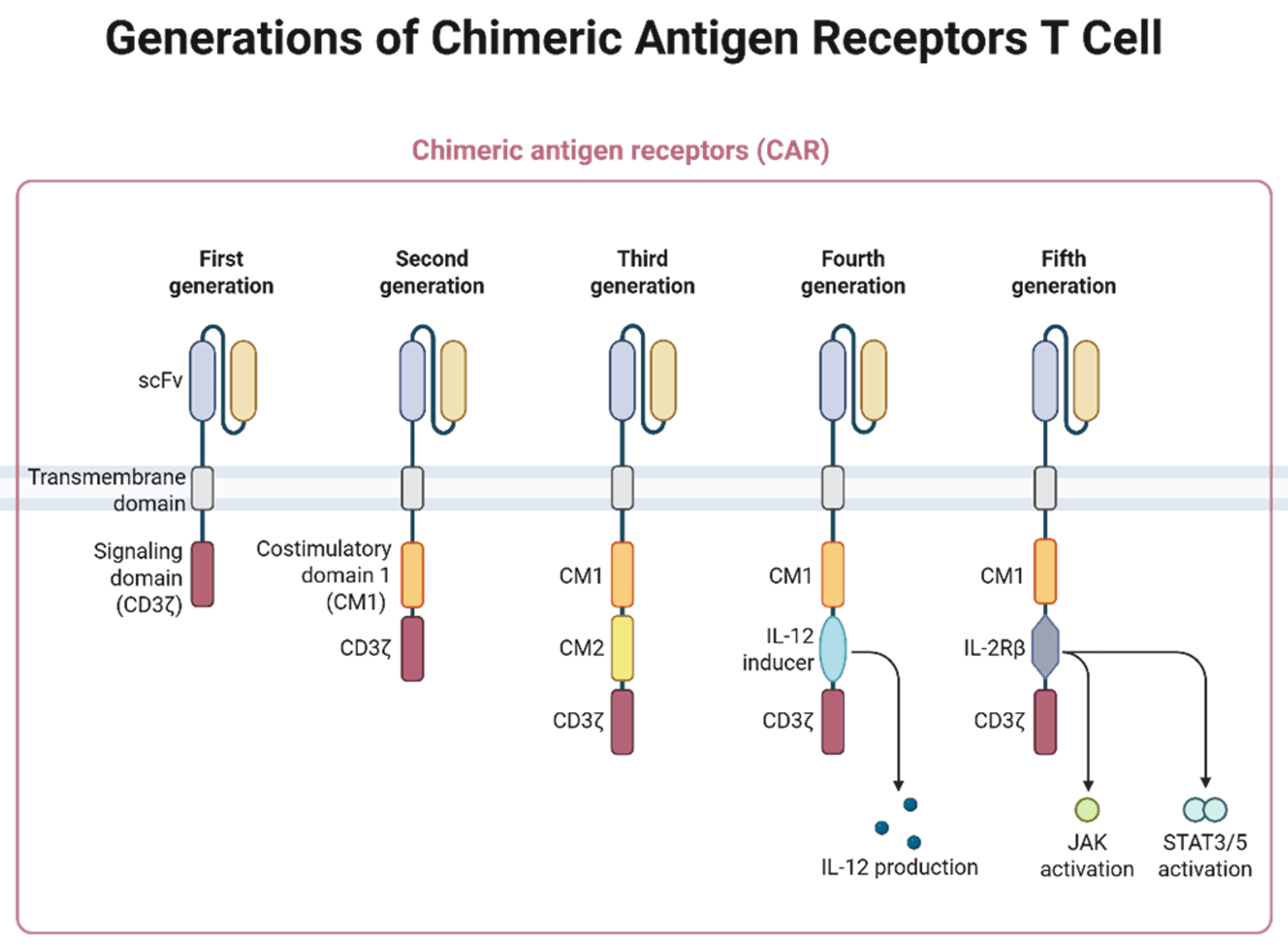
CAR-T cells are generated from T lymphocytes collected from patients, genetically engineered to express a CAR targeting at least one tumour antigen, then expanded and infused back to attack the patient cancer. This enables them to identify and eliminate cancer cells without reliance on major histocompatibility complex (MHC) presentation, a critical capability given that cancer cells frequently evade immune surveillance by downregulating MHC expression. The term "chimeric" in CAR refers to the fusion of an antibody-derived antigen-binding domain with T cell signalling regions, which serve to activate the T cell.
At RoukenBio, our specialists design, engineer, produce and characterise CAR-T cells for targeted immune cell therapies utilising our in-house CAR-T capabilities. Alternatively, our molecular biologists can design CAR constructs to your custom specifications.
The way CAR-T cells carry out their function can be divided into two stages:
When the binding region of the CAR recognises its target, the receptor clusters and activates intracellular signalling domains like CD3ζ, which are phosphorylated at ITAM sites. This triggers downstream signalling (e.g. ZAP-70 activation) leading to T-cell activation, proliferation, and cytokine release, all essential for initiating a robust immune attack against tumour cells.
Once activated, CAR-T cells kill tumour cells via multiple mechanisms:
Together, these processes ensure targeted and effective elimination of cancer cells, often with dramatic clinical outcomes. To make CAR-T therapies viable in more indications, especially solid tumours, researchers are developing strategies to overcome four major challenges: immunosuppressive TME, antigen specificity, resistance, and targeted delivery.
While CAR-T cell therapy has delivered remarkable results in blood cancers in recent years, its broader success in solid tumours, faces several biological and engineering hurdles. Researchers are actively developing CAR-T technologies to overcome these obstacles through innovative molecular designs and combination strategies. Let’s have a quick look at these challenges.
One of the biggest challenges for CAR-T therapies in solid tumours is the immunosuppressive TME. Unlike blood cancers, solid tumours often present complex defence systems that actively inhibit T cell function. This includes the recruitment of regulatory T cells (Tregs) and myeloid-derived suppressor cells (MDSCs), as well as the secretion of immunosuppressive cytokines like TGF‑β and IL‑10. Tumour cells may also express checkpoint ligands such as PD‑L1, which dampen T-cell activation.
To counteract these, scientists are:
Another major obstacle is tumour heterogeneity, more specifically the variation in antigen expression levels and density both within and between tumours. Furthermore, one major related challenge is the risk of on-target, off-tumour (OTOT) toxicity when healthy tissues express low levels of the target antigen. To navigate these, CARs are now being engineered with logic gating systems that act like molecular decision-makers:
Tumours are adaptive and may escape immune pressure by shedding or mutating the target antigen. For example, BCMA, a key target in multiple myeloma, can be cleaved from the cell surface by γ-secretase, leading to antigen loss and therapy resistance11.
To address this, researchers are exploring combination therapies, such as pairing BCMA CAR-T cells with γ-secretase inhibitors, to increase antigen density on tumour cells and reduce the risk of relapse12.
Finally, effective delivery of CAR T cells to solid tumours remains a major hurdle due to poor infiltration and physical barriers within the tumour mass. Innovative bioengineering approaches are being tested to enhance local delivery and retention:
Safety and Side Effects: CAR-T therapy can trigger acute toxicities such as cytokine release syndrome (CRS), which ranges from mild to life-threatening and may require intensive care. Early trials saw high rates of severe CRS, but improved protocols and early use of tocilizumab have reduced incidence to about 10–20% in some cases15. Neurotoxicity (ICANS), including confusion or seizures, occurs in 20–50% of patients but is often manageable with monitoring and steroids16. Most patients recover without long-term effects, and treatment-related mortality is under 3% at experienced centres. Due to these risks, CAR-T is restricted to hospitals with ICU support and requires close patient monitoring15,16.
Manufacturing, Cost, and Access: CAR-T therapy requires complex, individualised production that takes 1–2 weeks per patient, leading to high costs ($375,000–$600,000+) and limited availability17. Insurance may help, but affordability and access are major issues, especially outside wealthy countries and specialised centres. Travel and manufacturing delays can affect outcomes. Regulators face challenges ensuring quality and timely approvals, while ethical concerns about fair access, ongoing monitoring, and informed consent persist. Streamlining production and reducing costs are essential for broader use18.
The next steps for CAR-T therapies aim to expand their use, enhance safety, and lower costs. A major innovation is developing allogeneic, "off-the-shelf" CAR-T cells from donors, modified with gene-editing tools like TALEN or CRISPR to minimise immune issues19. These treatments are in early trials and could offer faster, more affordable access. Another exciting strategy under investigation is in vivo CAR-T generation, where vectors delivered directly to patients reprogram T cells inside the body, potentially streamlining treatment further, though this method remains largely experimental20.
New cell therapy platforms are emerging, such as CAR-NK cells, which use engineered Natural Killer cells that can kill tumours with potentially fewer side effects and allogeneic compatibility. Early trials in leukaemia and lymphoma show promising results for CAR-NK21, and other approaches like CAR-macrophages and TCR-engineered T cells are being studied22. The first approval of TIL therapy for melanoma in 202223 has increased optimism for adapting CAR-T to solid tumours.
As CAR-T therapy becomes more widely adopted, clinicians are testing its use earlier in treatment, including replacing second transplants or serving as a frontline option for high-risk cases. Studies like ZUMA-12 have shown high response rates when CAR-T is used initially in aggressive cancers24. Efforts are ongoing to make CAR-T safer and more accessible, including outpatient administration and improved toxicity management.
Experts acknowledge that CAR-T is not a panacea, and continuous research is critical to tackle its current limitations. Key areas of active research include improving CAR-T cell persistence and exhaustion, identifying better tumour antigens (especially for solid cancers), enhancing manufacturing efficiency, and managing immune side effects with greater precision.
In June 2025, Gilead and University of Pennsylvania reported promising results for a novel CAR-T cell therapy targeting recurrent glioblastoma25. Tumours shrank in 62% of evaluable patients, with manageable neurotoxicity and some patients achieving stability beyond 6 months. The CAR targeted both EGFR and IL‑13Rα2.
At ASCO 2025, a randomised trial in advanced gastric and gastro‑oesophageal junction cancers showed CAR-T cell therapy extended survival by around 40%26, a milestone road‑map for solid tumour application. The CAR targeted CLDN18.2 positive gastric or gastroesophageal junction cancer.
CAR-T cell therapy is transforming cancer treatment, showing strong results in blood cancers and progress with solid tumours. Advances in engineering are addressing challenges like tumour heterogeneity and delivery. While there are safety, cost, and access issues, ongoing innovations (including allogeneic and in vivo platforms) are making these therapies safer and more available. Recent clinical and technological breakthroughs suggest CAR-T could soon become a standard option for more cancers, supported by continued research and collaboration.

Access the CAR-T slides
🗓️ Stay informed with our monthly scientific newsletter, published on LinkedIn on the last Wednesday of each month.
These editions bring you the latest in drug development breakthroughs, industry trends, and expert insights from the brilliant minds at RoukenBio.
Subscribe today on LinkedInAre you developing the next breakthrough in CAR T cell therapy? Discover how our expertise can accelerate your journey. Explore two real-world CAR T case studies and learn how our platforms and capabilities are designed to support cutting-edge cell therapy development.

 Webinars
Webinars Insights
Insights Whitepapers
Whitepapers